 English
English Deutsch
Deutsch
Call Us
TEl: +86-13148388090
Fax:+86-571-88616515

Airway management in anesthesia refers to managing the patient's airway so that he/she has an open airway for adequate ventilation and oxygenation during anesthesia. There are medical tools designed and used for this purpose.
When we talk about airway management in anesthesia, the subject prompts a logically relevant question: How is the patient's airway affected during anesthesia?
The patient’s airways can be affected during anesthesia in the following ways.
Anesthetics can depress the respiratory centers in the brainstem, reducing or completely inhibiting the patient's spontaneous breathing. This suppression can to hypoventilation (inadequate ventilation) or apnea (cessation of breathing), making it necessary for the anesthesia provider to manage the patient's ventilation through medical devices such as a mechanical ventilator.
Anesthetic agents, especially general anesthetics, suppress the central nervous system. This suppression leads to the loss of protective reflexes such as coughing, gagging, and swallowing, which normally help keep the airway clear and prevent the aspiration of foreign materials. The absence of these reflexes increases the risk of aspiration of gastric contents or other substances into the lungs.
In this case, an endotracheal tube is the commonly used medical airway management device because the primary purpose of using an endotracheal tube is to secure the airway and protect the lungs from aspiration. For expert information and specifications of endotracheal tubes, you can refer to a specialized manufacturer such as this one: www.bevermedical.com (Hangzhou Bever Medical Device Co., Ltd.)
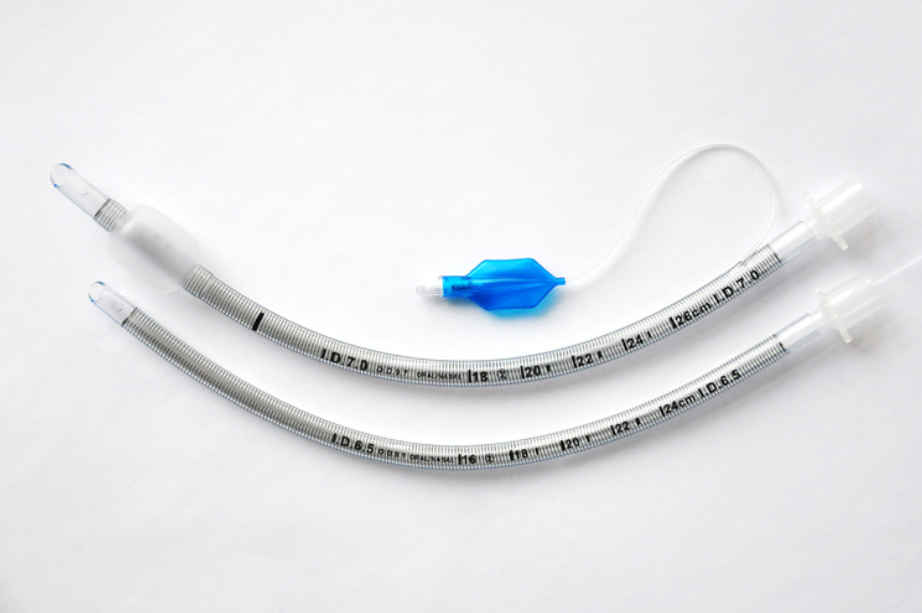
Endotracheal tube from Hangzhou Bever Medical Device
General anesthesia often involves muscle relaxants, which relax the muscles of the body, including those in the upper airway. This relaxation can to a loss of muscle tone in the tongue, soft palate, and pharyngeal muscles, potentially causing airway collapse. In particular, the tongue may fall back against the posterior pharynx, obstructing the airway.
In this case, a nasopharyngeal airway can be used to solve the problem. It is an adjunct used to keep the airway open by preventing the tongue from falling back and obstructing the airway.
To give you a vivid idea of what it is, the following is an illustrative image of it.

Nasopharyngeal airways from Hangzhou Bever Medical Device
Some of the common medical devices used in airway management during anesthesia are a mechanical ventilator, an endotracheal tube (ETT), and a nasopharyngeal airway mentioned above. They can all ensure adequate ventilation and airway patency. The following is a detailed explanation of how each device is used.
1) Mechanical ventilator
The mechanical ventilator is connected to the patient via an endotracheal tube (ETT). The ventilator delivers controlled breaths to the patient, ensuring sufficient oxygenation and removal of carbon dioxide.
The ventilator continuously monitors and adjusts the delivery of breaths based on preset parameters and patient needs. It helps in managing the patient's ventilation during surgeries under general anesthesia and can be adjusted according to the patient's condition and surgical requirements.
2) Endotracheal tube (ETT)
(1) Insertion: The ETT is inserted through the patient's mouth (or occasionally through the nose) and advanced into the trachea. The procedure is often performed after administering anesthetic agents and muscle relaxants to facilitate intubation.
(2) Cuff Inflation: Once in place, the cuff at the end of the ETT is inflated to create a seal against the tracheal wall. This prevents air leaks and protects against aspiration of stomach contents.
Notes:
The cuff is a small inflatable balloon located at the end of the ETT. The primary function of the cuff is to create a seal between the tube and the tracheal walls. This seal prevents air from leaking around the tube. The cuff also helps prevent the aspiration of gastric contents, secretions, or other fluids into the lungs. By sealing the airway, it provides a barrier that reduces the risk of aspiration pneumonia.
(3) Connection to Ventilator: The ETT is connected to a mechanical ventilator or a manual ventilation device (e.g., bag-valve mask) to provide controlled breathing and ensure adequate ventilation during anesthesia.
3) Nasopharyngeal Airway
A nasopharyngeal airway is used to maintain airway patency by preventing obstruction caused by the tongue or other soft tissues in the upper airway.
(1) The nasopharyngeal airway is a soft, flexible tube inserted through the patient's nostril and advanced into the nasopharynx.
(2) Size Selection: The size of the nasopharyngeal airway is chosen based on the patient's age and anatomy. It should be sized appropriately to ensure effectiveness and minimize discomfort.
A nasopharyngeal airway is used in situations where full intubation is not necessary.
4) Other medical devices available in addition to the above three devices
Besides the three medical devices described above, the oropharyngeal airway (OPA) is another airway management option. OPA is a simple, non-invasive device used in airway management to maintain a patent airway by preventing the tongue and soft tissues from obstructing the pharynx. It is commonly used during anesthesia and in emergencies.
During anesthesia, especially when muscle relaxants are used, the muscles of the upper airway can relax, causing the tongue to fall back and obstruct the airway. The OPA helps to keep the airway open by mechanically displacing the tongue away from the posterior pharyngeal wall.
NPAs are contraindicated in patients with nasal trauma, fractures, or deformities. The insertion of an NPA can exacerbate these conditions or cause further injury. In such cases, an OPA is a safer alternative.
We hope this article addresses the question you may have about how exactly health professionals handle airway management in anesthesia. It is our pleasure if our articles contribute to the promotion of understanding of healthcare practices for patients or their concerned families and friends.
Copyright © Hangzhou BEVER Medical Devices Co., Ltd.
The information provided on this website is intended for use only in countries and jurisdictions outside of the People's Republic of China.
